 © Lester Ledesma / Asian Development Bank
© Lester Ledesma / Asian Development Bank
Biodiversity and Infectious Diseases: Questions and Answers
Infectious diseases cause over one billion human infections per year, with millions of deaths each year globally. Extensive health and financial burden is seen from both established and emerging infectious diseases. Infectious diseases also affect plants and animals, which may pose threats to agriculture and water supplies with additional impacts on human health. This Question and Answers, prepared by the World Health Organization (WHO) and Convention on Biological Diversity (CBD) Secretariat under their joint work programme on biodiversity and health, and launched of the occasion of the International Day for Biodiversity 2020, summarizes some of the interlinkages between biodiversity and infectious diseases.
WHO is continuously monitoring and responding to the COVID 19 outbreak. This Q&A will be updated as more is known about COVID-19, how it is affecting people worldwide, and the effectiveness of interventions against the disease
A PDF version of this document can also be downloaded here.
Questions and Answers
We depend on biodiversity and healthy ecosystems for our health and survival. Biodiversity, and the complexity of our landscapes and seascapes, is integral to social and ecological resilience, including the resilience of ecosystem functions and the services that they sustain. As genetic and species diversity is lost and ecosystems are degraded, the complexity of the overall system can be compromised making it more vulnerable, and potentially creating new opportunities for disease emergence and poor health outcomes both in humans and species.
Biodiversity is declining globally at unprecedented rates in human history, and the rate of species extinctions is accelerating, impacting human health worldwide in a variety of ways. The global assessment of the Intergovernmental Science-Policy Platform on Biodiversity and Ecosystem Services (IPBES) demonstrated that ecosystems are being degraded at unprecedented rates. For example, three-quarters of the land-based environment and about two-thirds of the marine environment have been significantly altered by human actions. At the same time, over a third of the world’s land surface and nearly 75% of freshwater resources are now devoted to crop or livestock production. Combined, these and other drivers, including climate change, are jeopardizing the health, livelihoods and well-being of hundreds of millions of people globally.
Often, the least affluent and most vulnerable segments of society are also the most directly reliant on biodiversity for their livelihoods, health and well-being. They are also often the least responsible for biodiversity loss and least covered by social protection mechanisms, including access to healthcare, once diseases emerge.
Healthy communities rely on well-functioning and biodiverse ecosystems. These provide clean air, fresh water, medicines, food and nutrition security and support critical ecosystem functions and services such pest and disease regulation, pollination, climate regulation, and mitigating the impacts of extreme events. The availability and sustainable management of natural resources in large part determines the baseline health status of a community, securing livelihoods and warranting community resilience. Healthy and biodiverse ecosystems also limit the emergence and spread of disease and stabilize the climate.
Biodiversity is also an important source of genetic resources for the development of many treatments, vaccines and a range of biotechnology products used in both modern and traditional medicines, as well as agriculture and industry. These include, for example, artemisinin as a treatment for malaria, and digitalis for heart disease.
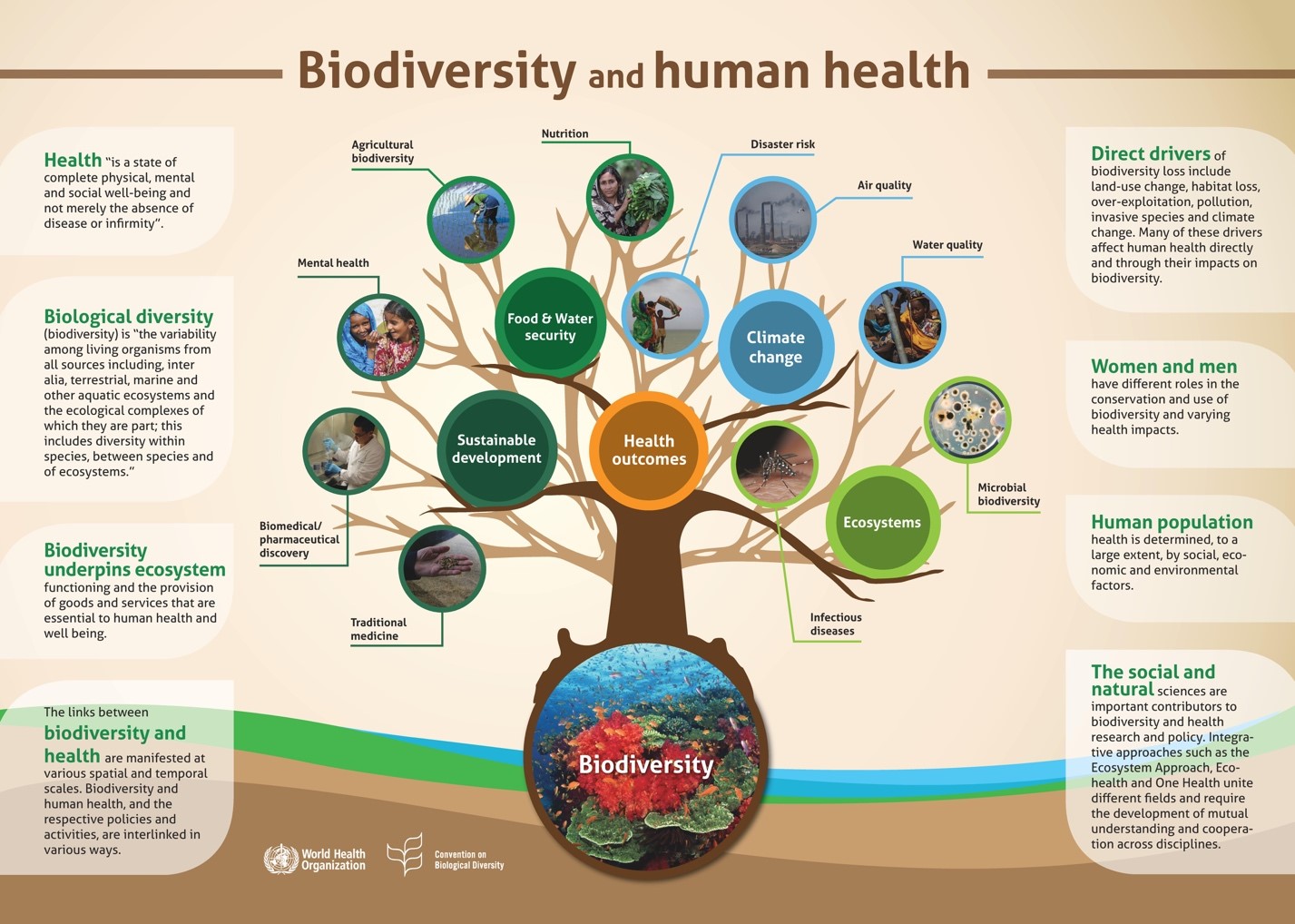
The infographic below, from the WHO and CBD led State of Knowledge Review, Connecting Global Priorities Biodiversity and Human Health, provides a visual representation of some of the interconnections between biodiversity and health.
Biodiversity loss, ecosystem degradation and disease share many common drivers. Human disturbance of ecosystems and biodiversity loss are increasingly linked to the occurrence and risk of diseases spread of zoonotic and vector-borne diseases. In many instances, climate change acts as a threat multiplier. Changing weather patterns can shift the geographic range, seasonality, and intensity of transmission of some climate-sensitive diseases, particularly vector-borne diseases.
Changes in land-use (e.g. land conversion, oil extraction, mining, deforestation, wetland drainage, etc.) and food production practices, have been identified as the leading driver of emerging infectious diseases. Changes in habitat can alter species distribution, abundance, movement, interactions with other species, with corresponding implications for immune responses and disease emergence. Other human disturbances to ecosystems that affect the emergence of infectious diseases include: deforestation; water management processes (e.g. through dam construction); urbanization; the use of pesticides and antimicrobials; climate change; migration and international travel and trade; and the accidental or intentional human introduction of species that carry pathogens.
Such human disturbances to natural ecosystems affect patterns of infectious diseases by reducing the abundance of some organisms, causing population growth in others, modifying some interactions among organisms, and altering interactions between organisms and interactions between biotic (e.g., animal, plants, fungi, bacteria) and abiotic (e.g., temperature, water, air, sunlight) components of the environment.
The Table below provides an overview of ways in which human-caused environmental changes can influence the emergence, occurrence or risk of certain infectious diseases. It is important to note that infectious diseases arise from a combination of ecological, social and economic pressures that combine to amplify disease risk, rather than any individual driver acting in isolation.
TABLE: Examples of anthropogenic environmental changes that affect the emergence, occurrence or risk of infectious diseases
Type of environmental Change |
Example Disease |
Pathway of risk change |
|---|---|---|
|
Agricultural intensification |
Malaria |
Crop insecticides and increased vector resistance |
|
|
Venezuelan heamorraghic fever |
Increased rodent abundance, contact |
|
Global temperature rise |
Malaria, Dengue fever, Chikungunya, Yellow fever, Zika |
Increased number and range of vector mosquitos |
|
|
Lyme disease |
Increased number and range of tick vector |
|
Deforestation and habitat encroachment |
Malaria |
Increased breeding sites and vectors, migration of susceptible people |
|
|
Oropouche |
Increased contact, breeding of vectors |
|
|
Visceral leishmaniasis |
Increased contact with sandfly vectors |
|
|
Ebola virus disease |
Increased contact and pathogen transmission with infected animals |
|
|
Avian influenza H5N1, H7N9 |
Increased contact and pathogen transmission among captive birds, wild birds and people |
|
|
H1N1 virus disease, Nipah virus disease |
Increased contact among captive pigs and people |
|
Dams, canals, irrigation |
Schistosomiasis |
Increased snail host habitat, human contact, habitat destruction |
|
|
Malaria |
Increased breeding sites for mosquitoes |
|
|
Helminthiasis |
Increased larval contact due to soil moist |
|
|
River Blindness |
Decline in blackfly breeding, decline in disease |
|
Urbanization |
Cholera |
Decline sanitation, hygiene, Increased water contamination |
|
|
Dengue |
Increased water-collecting trash, Increased Aedes mosquito breeding sites |
|
|
Cutaneous leishmaniasis |
Increased proximity, sandfly vectors |
|
Habitat fragmentation |
Lyme disease |
Increased tick hosts, outdoor exposure, increased contact in fragmented landscapes |
|
Ocean warming |
Red tide |
Increased toxic algal blooms |
|
Increased precipitation |
Rift valley fever |
Increased pools for mosquito breeding |
|
|
Hantavirus pulmonary syndrome |
Increased rodent food, habitat, abundance |
|
Wildlife trade or -breeding |
HIV, monkeypox, SARS |
Increased contact among captive animals and people |
Infectious disseases include zoonotic and vector-borne diseases. A zoonosis is any disease or infection that is transmissible from animals to humans. Zoonoses may be caused by viruses, bacteria, or parasitic animals (such as protozoa (singe celled-organisms), helminths and arthropods. Over 60% of known human infectious diseases reported globally are zoonotic. As well as being a public health problem, many of the major zoonotic diseases also affect animal populations.
There are three classes of infectious diseases: a) endemic: which are present in many places and affect many people and animals; b) epidemic: which are sporadic in temporal and spatial distribution; and c) emerging and re-emerging infectious diseases which either appeared and affected a population for the first time, or have existed previously but are rapidly spreading, either in terms of the number of people getting infected, or to new geographical areas.
Vector-borne diseases are human illnesses caused by parasites, viruses or bacteria that are transmitted by vectors (e.g. Anopheles mosquitoes which can transmit malaria to humans). Every year there are more than 700,000 deaths from vector-borne diseases such as malaria, dengue, schistosomiasis, leishmaniasis, Chagas disease, yellow fever, and Japanese encephalitis.
The burden of these diseases is highest in tropical and subtropical areas, and they disproportionately affect the poorest populations.
The number of emerging infectious disease outbreaks has increased steadily since 1980.
up to 75% of new or emerging infectious diseases are zoonotic in origin. Emerging infectious diseases have potentially serious human health and economic impacts and their current upward trends are likely to continue.
The majority of new, emerging, or re-emerging diseases affecting people are of zoonotic origins (i.e., they existed naturally in animals) before spilling over to other species, including humans. Examples include AIDS, SARS, MERS, Nipah Virus, Avian influenza, Ebola virus disease and Influenza A virus subtype H1N1 disease, as well as COVID-19.
Vector-borne diseases such as Malaria, Zika virus disease, dengue, West Nile Virus, chikungunya, and yellow fever also account for a large share of endemic diseases, accounting for more than 17% of all infectious diseases. Anthropogenic activity is changing vector abundance, composition, and/or distribution, including through the effects of climate change.
Infectious diseases, both zoonotic and vector-borne, are a significant cause of disability and mortality worldwide, resulting in over one billion human infections and over one million deaths every year. They disproportionately impact citizens of low- and middle- income countries and other vulnerable populations.
Pathogen spillover occurs when a pathogen endemic to one host species infects a new host species (i.e. animal or human), either directly or through an intermediate host species. The emergence of zoonotic diseases can be considered a consequence of pathogen ecology and evolution, as pathogens exploit new niches and adapt to new hosts.
Human activity and environmentally destructive practices are also changing pathogen dynamics. While pathogen evolution is a natural phenomenon, factors such as global travel, climate change, and overuse and misuse of antimicrobial agents can influence pathogen movement, host ranges, and persistence and virulence. Beyond direct infection risks for human and animals, such changes also have implications for food security, nutrition, medicine and other dimensions of health.
Many factors contribute to the process of cross-species transmission in animal and human populations. While all the underlying mechanisms are not fully understood it is well established that these include environmental changes, such as land-use change, human and animal demography, pathogen changes and changes in farming practice, as well as economic, social and cultural factors (e.g. trade, travel, food habits).
Sometimes. The potential of human-to-human transmission of enzootic diseases varies among pathogens. Some infections can be transmitted from animals to people, but typically do not transmit between people (e.g. rabies), whereas others may be maintained in human populations primarily by human-to-human transmission following an initial infection (as is the case with Ebola virus disease, Rift Valley fever, severe acute respiratory syndrome (SARS), and HIV, , as well as COVID-19, among others).
Stressed environmental conditions can significantly alter disease patterns of emerging and re-emerging infectious diseases, and compromise the resilience of the system as a whole.
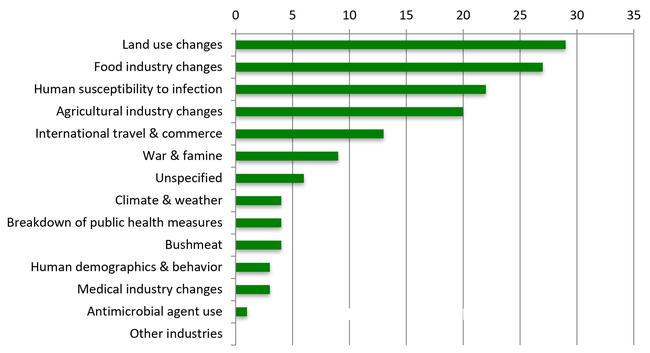
Most emerging infectious diseases —whether in wildlife, domestic animals, plants or people — are driven by human activities such as agricultural intensification and human- induced landscape changes, interacting in a co-evolutionary process and with other drivers such as trade and travel which facilitate disease spread once spillover has occurred. Some of the primary drivers of emerging infectious diseases are summarized below.
Drivers of recently-emerging infectious diseases in humans (in %)
Yes. Coronaviruses are a large family of viruses that are common in animals. Several coronaviruses cause respiratory diseases in humans, from the common cold to more rare diseases such as the Severe Acute Respiratory Syndrome (SARS) and the Middle East respiratory syndrome (MERS), both of which have high mortality rates and were detected for the first time in 2003 and 2012, respectively. Both diseases emerged from a zoonotic pathogen. Spillover into human populations of the SARS coronavirus has been associated with civet cats, while the MERS coronavirus is transmitted by dromedary camels.
The current COVID-19 pandemic is caused by a coronavirus named SARS-CoV-2.
The first human cases of COVID-19, the coronavirus disease caused by SARS-CoV-2, were first reported from Wuhan City, China, in December 2019. Currently, the zoonotic source of SARS-CoV-2 is unknown. However, SARS-CoV-2, the virus responsible for COVID-19, belongs to a group of genetically related viruses that includes SARS-CoV and a number of other coronaviruses isolated from bat populations from the genus Rhinolophus. These close genetic relations suggest SARS-CoV and SARS-CoV-2 have their origin in bat populations. MERS-CoV also belongs to this group of viruses but is less closely related.
When a new virus is discovered, it is important to identify and isolate the source and prevent further introductions of the virus into the human population, as well as animal populations, as applicable. It also helps to understand the dynamic of the beginning of the outbreak, which can be used to inform the public health response. Understanding the origin of the virus may also aid the development of therapeutics and vaccines.
To identify the source or origin of a virus, it is helpful to look at the genetic makeup of the virus and see whether it resembles other known viruses. This may provide some clues as to its origin. Viruses that are genetically closely linked tend to come from a similar source or similar geographic area.
Wet markets are not synonymous with wildlife markets or live animal markets. What are known as “wet markets” in parts of Asia, are markets in which fresh fish, seafood, meat, poultry, other fresh produce and, occasionally, wild animals are also sold. Some include live animal markets. Some such practices can be a risk factor for the emergence and spread of disease, as is the global trade of wildlife.
Measures to reduce or eliminate the presence of wildlife species in food markets, to apply stringent food safety and hygiene standards and to rigorously inspect live animal markets and breeding facilities for captive wild animals all have the potential to significantly reduce the risk of future disease outbreaks. In addition, targeted behavioural measures, strict controls on illegal wildlife trade and more stringent regulations on the sale and consumption of wild animal species are essential measures for the prevention of future disease outbreaks.
No individual measure will be sufficient to eliminate the risk of zoonotic diseases from the unsafe handling, trade and consumption of wildlife. Careful evaluation of an integrated package of measures, including community education and awareness raising, is needed to reduce the unintended consequences that may arise from blanket measures.
The sale and consumption of wild species sustain the livelihoods of millions of people globally. Wild plant and animal species are also a critical source of food security and nutrition, especially among people living in low-income countries or in remote areas. A blanket ban on live animal markets and the trade, farming and consumption of wild species would not, on its own, necessarily eliminate the risk of future zoonotic spillover of diseases and, under some conditions, it may even generate new opportunities for diseases to emerge. Unintended consequences of a blanket ban on wildlife trade and markets may include increasing illegal wildlife traffic, as occurred when bans were temporarily attempted in 2003, in response to the SARS outbreak, and in 2013-2014, in response to an outbreak of avian influenza H7N9. Importantly, a global ban may also potentially jeopardize the livelihoods of many smallholder farmers who rely on informal supply chains for income.
Regulations on wildlife trade and live animal markets therefore need to be thoughtful of socio-economic dependencies and cultural and societal circumstances to be effective and sustainable.
Current negative trends in biodiversity and ecosystems will undermine progress towards 80% (35 out of 44) of the assessed targets of the Sustainable Development Goals, related to poverty, hunger, health, water, cities, climate, oceans and land (SDGs 1, 2, 3, 6, 11, 13, 14 and 15).
The Global Assessment report of the Intergovernmental Science-Policy Platform on Biodiversity and Ecosystem Services (IPBES) found that global goals for conserving and sustainably using nature cannot be met by current trajectories. The assessment highlighted that biodiversity and developmental goals for 2030 and beyond can only be achieved through transformative changes across economic, social, political and technological factors.
More robust, comprehensive and coordinated detection, prevention and control strategies are needed to protect people from the health impacts of environmental disaster and disease emergence and spread. This includes through coordinated, cross-sectoral approaches such as One Health.
The Food and Agriculture Organization (FAO), World Organization for Animal Health (OIE) and WHO also define and regularly update guidelines for good practices, methods, tools and strategies for infectious diseases, focusing on developing countries and/or endemic areas. As a way to support countries in taking a One Health approach to address zoonotic diseases, the guide: “Taking a Multisectoral, One Health Approach: A Tripartite Guide to Addressing Zoonotic Diseases in Countries” was developed in 2019.
It is critical that countries have the capacity to detect, assess, and respond to public health crises. The International Health Regulations (IHR) are intended to help the international community prevent and respond to acute public health risks. In addition to the IHR, several voluntary guidelines that have been adopted should also be encouraged as a prevention measure.
The Codex Alimentarius,shared by FAO and WHO, develops food and feed standards and provides guidelines and codes of practice with the aim of protecting the health of consumers, ensuring fair food trade practices, and promoting the coordination of all work around food standards undertaken by intergovernmental organizations and NGOs.
Other examples include the OIE Tool for the Evaluation of Performance of Veterinary Services (OIE PVS Tool). A similar tool is also available for the evaluation of Aquatic Animal Health Services.
The Conference of the Parties to the Convention on Biological Diversity also adopted also adopted a biodiversity-inclusive One Health guidance as a means to ensure the integration of biodiversity into integrated, cross-sectoral approaches such as One Health.
The International Health Regulations, represents a binding international legal agreement involving 196 countries across the globe, including all the Member States of WHO. The IHR is the only binding global legal instrument dedicated to the prevention and control of infectious diseases. The aim of the IHR is to help the international community prevent and respond to acute public health risks that have the potential to cross borders and threaten people worldwide. The purpose and scope of the IHR is to prevent, protect against, control and provide a public health response to the international spread of disease in ways that are commensurate with and restricted to public health risks, and which avoid unnecessary interference with international traffic and trade.
The Joint External Evaluation (JEE) is a voluntary component of the IHR monitoring and evaluation framework. It is a voluntary, collaborative, multisectoral process to assess country capacities to prevent, detect and rapidly respond to public health risks. The JEE helps countries identify critical gaps within their human and animal health systems in order to prioritize opportunities for enhanced preparedness and response.
One Health and other integrated approaches recognize that human health is intimately connected to the health of animals and our shared environment, as well as socio- economic and political factors. It brings together essential expertise from multiple sectors and fields including epidemiology, public health, ecology, veterinary medicine, economics, and sociology, among others. Strengthening cross-sectoral collaboration, partnerships and data sharing among relevant sectors (e.g., public health, environment, agriculture) and stakeholders, investing in active monitoring and surveillance and early warning systems and carrying out integrated impact and risk assessments are all important components of One Health.
Integrated approaches to health are foundational pillars of prevention and early detection of health risks. Investing in prevention and early warning systems is imperative and far less costly (from both a human and economic perspective), than emergency response once an epidemic has emerged.
At the local, national and global scale, the implementation of One Health approaches has led to improved outbreak responses, generated critical data, contributed to the discovery of new pathogens, informed disease control programs to reduce burden of diseases and enhanced preparedness for infectious diseases.
Surveillance and reporting employing a One Health approach may provide sentinel benefits to enable early detection of potential pathogens that could spill over from wild animal species and livestock to humans. This is especially important given chronic under- reporting of disease in animals, including in food production, as well as changing ecological factors.
Past Ebola virus outbreaks in great apes, for example, have preceded human outbreaks, suggesting a sentinel or predictive value of wildlife monitoring to aid in early detection or prevention of human infections. Strengthening collaboration on surveillance and data- sharing between human health, agriculture, environment and other sectors promotes a more comprehensive approach in preventing and responding to health risks, now and in the future.
At the global level, has been increasingly recognized and adopted by international organizations including the WHO, Food and Agriculture Organization of the United Nations (FAO), World Organization for Animal Health (OIE), as well as the Convention on Biological Diversity (CBD).
There are various applications of One Health approaches, with varying degrees of integration of the environmental sector and ecosystem health. Given the relevance of ecosystem dynamics to infectious disease emergence, efforts have been made to ensure that these are more systematically incorporated in One Health approaches. Building on the findings of the State of Knowledge Review on biodiversity and health, and on the need for inclusive multi-sectoral approaches to address global health challenges, in 2018, the Conference of the Parties to the CBD also adopted a biodiversity-inclusive One Health guidance.
At the national level, some countries have an existing government ministry, department, or agency with a multisectoral coordination mechanism to respond to zoonoses or potential zoonoses, antimicrobial resistance, and coordination efforts involving the International Health Regulations . While One Health can make an important contribution to global health security, it remains underfunded and relatively few countries have formal mechanisms in place.
For more information on COVID-19, please visit the WHO COVID-19 website.
This briefing note was jointly produced by the WHO and CBD Secretariat as a product of their collaboration under the Joint Work Programme on biodiversity and health.
For more information on the WHO & CBD Joint Work Programme, and related activities, please visit the following websites:
- https://www.who.int/news-room/detail/01-01-2020-biodiversity-and-health-the-who-cbd- joint-work-programme
- https://www.cbd.int/health/
- https://www.unbiodiversityandhealth.com/
In collaboration with the University of Geneva, and other partners, WHO and the CBD Secretariat have also prepared a ten-part module on biodiversity and health for the course Global Health at the Human Animal Ecosystem Interface.
For more information and to sign up for the online course please visit:
You can view the course trailer here.